
Completing TTAs (To Take Away) medications and writing a discharge summary (or a discharge letter) is a core skill in the NHS that a junior doctor must master.
Multiple teams start discharge planning once the patient is MSFD (Medically Stable For Discharge). As part of the medical team, your duty also involves completing a discharge letter, sending a copy to the GP, and giving it to the patient or their family if they ask.
So, what constitutes a good discharge summary? How do you write one? What are the steps? We will break it down so it is easier for you to understand.
What is a Discharge Summary?
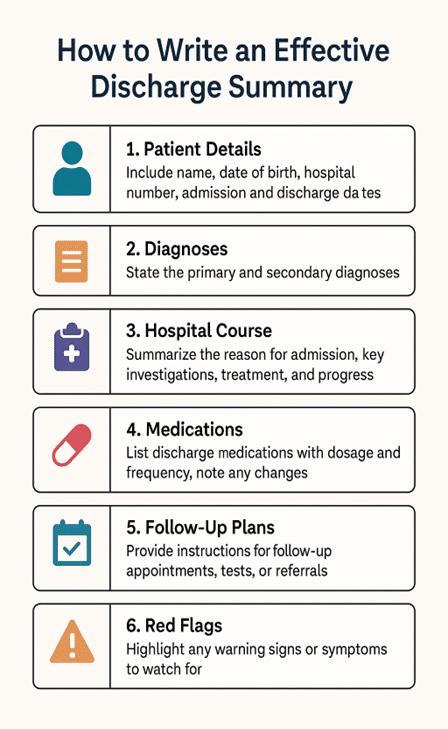
A discharge letter, also known as a discharge summary, is a medical document that is written when a patient leaves the hospital. It has:
- A summary of the admission
- Diagnoses and important treatments
- Results of the investigation
- Appointments for outpatients
- Instructions for follow-up
- A list of medications with changes
- Contact information for ongoing care
It’s sent to the GP practice and sometimes shared with patients, social care teams, and community services.
Why Discharge Summaries Matter
Many healthcare professionals, mainly GPs (general practitioners) and others such as community nurses, pharmacists, and patients, rely on discharge letters to understand what happened and what needs to be done next.
An unclear or incomplete discharge summary can lead to missed appointments, medication errors or delays in the treatment. On the other hand, a clear, concise and well-written summary can help understand key concerns and next steps easily and can directly improve the patient’s outcomes after discharge.
When properly completed, a hospital discharge letter helps guarantee:
- Smooth continuity of care
- Good communication between general practitioners and hospital staff
- Fewer mistakes and safer follow-up
- Reduced readmissions
- Improved comprehension and trust among patients
NHS Discharge Letter Templates
Let’s start with a discharge summary template first, and then we will break down the structure.
Here is a discharge letter template used by NHS doctors in geriatric wards:
Dear Doctor,
Mr X, 68YO male, presented to the hospital with complaints of cough, fever, and chest pain and was admitted to the hospital on 03/08/2025.
Past Medical History: Hypertension, Type 2 diabetes mellitus
Social History: Lives alone in a house, twice a day carers, walks with a frame, ex-smoker, occasional alcohol, drives
AMT= 8/10
DNACPR in place
Initial diagnosis:
1. Community-acquired pneumonia
Examination revealed crackles in the chest. He was adequately hydrated and cognitively intact throughout admission.
Initial bloods revealed high inflammatory markers (CRP 80 and WCC 13.1). Electrolytes and kidney functions were normal.
He was started on intravenous antibiotics, supplemental oxygen, and analgesia.
Chest xray confirmed consolidation in the right side of the lung.
Over time, he was weaned off the oxygen, and his symptoms improved gradually.
The PT/OT assessed him before discharge, and a care plan was established.
Clinical frailty score was noted to be 6 on discharge as opposed to 5 two weeks ago.
He has been given 5 days of oral co-amoxiclav to complete the course of antibiotics.
He will be followed up in the frailty assessment unit in 6 weeks with a chest xray for further assessment.
At the time of discharge, his symptoms have improved, safety netting has been done, and he is medically optimised for discharge.
We wish him luck.
Best regards,
Care of the Elderly team,
xxx hospital
What do you see in this discharge summary? I will highlight all the points in this discharge summary template:
- Presenting complaints
- Admission date
- Past medical history
- Social history (important in elderly patients)
- AMT
- DNAR status
- Initial examination
- Significant bloods or related investigations
- Imaging including xrays and scans
- Treatment given and course of disease
- Assessment by MDT for discharge planning
- Clinical frailty score (again crucial in elderly patients)
- Medication changes, if any
- Further follow-ups
- Safety netting/ important points/ notes for GP

Writing a Discharge Letter with Examples
Here’s how to write an NHS discharge letter practically, with examples and easy steps you can follow. I will also highlight some key points in the sample summary that a doctor in the NHS must know.
Step 1: Patient Details
Usually pre-filled on the system, but I will mention it for quick understanding.
Patient Demographics
These include patient name, age/sex, address, next of kin details, hospital and NHS number, contact info, and GP details.
These are usually pre-filled and can be found at the top of the screen.
Admission Details
This is usually found on the first tab of your IT system. It consists of the date and time of admission, the admitting consultant, and a summary of the patient as seen on the take list.
Example:
Date of Admission: 20/07/2025
Time of Admission: 10:30 AM
Admitting consultant: Dr. Smith
Department of Admission: General Medicine
Reason for Admission (Presenting Complaint): 68YO male with CAP, on IV co-amoxiclav and clarithromycin, DNACPR in place
Step 2: Presenting Complaints
Start by explaining the reason for admission, which is often written by on-call doctor and found on the clerking proforma or A&E notes, or as a direct question from the patient or family.
Expand on anything significant and relevant. Mention the admission date, as sometimes IT systems can be unclear (especially if multiple admissions).
Pro tip: Sometimes, you will encounter confused patients, and it is not feasible to take history from them. In such a case, take history from family members or carers. If they are not available, you can still write- it is challenging to take history as confused, and complete your assessment and initial management plan.
Step 3: Past Medical History
Start with the ones that are linked to the presenting complaints. An example is COPD, where a patient presents with cough and fever, which helps plan treatment options such as steroids and nebulisers.
Step 4: Social History
This part of hospital discharge letter is often overlooked, but must be expanded and mentioned in patient groups such as the elderly.
For example, it is vital to know the driving status of an epilepsy patient, or mobility and support for elderly patients, as this will better help the occupational therapists and physiotherapists during the discharge planning.
Step 5: AMT
This is again relevant and important for confused patients, as this helps you create a plan to rule out medical and treatable causes of delirium. Furthermore, letter of discharge from hospital also allows the GP to follow up or repeat important bloods, such as electrolytes, after a few weeks if necessary.
Usually, a score above 6 is normal or mild cognitive impairment, but a score below 6 triggers a need for a confusion screen assessment.
Step 6: DNAR Status
If you have ever worked in the NHS, you know how critical it is to understand the DNACPR status and the TEP (Treatment Escalation Plan) of the patient.
This not only helps plan further steps such as escalation to HDU or ward-based care but also guides the medical team in making decisions in the best interest of the patient.
Step 7: Initial Examination
Highlight systemic examination, general inspection points (for example, frail patient, confused, agitated, etc.). This gives a general idea of the initial status of the patient.
You can also mention the NEWS2 score if necessary.
Example:
On admission, the patient was febrile (T 38.6°C), tachypneic with RR 24, and SpO₂ 91% on room air. Chest auscultation revealed crepitations over the left lower zone. BP was 138/84 mmHg, pulse 102 bpm. Cardiovascular and abdominal exams were unremarkable.
Step 8: Investigations
Significant Bloods and Related Investigations
If you plan to enter all the bloods, the discharge letter can look chaotic. Instead, mention the abnormal bloods or related investigations such as blood culture, viral screen, sputum mc&s, urine dipstick and culture, etc.
Example:
WCC 18.5 ×10⁹/L (neutrophil predominant), CRP 150 mg/L
Hb 11.8 g/dL, Platelets 320 ×10⁹/L
RBS 280 mg/dL
U&Es and LFTs within normal limits
Sputum mc&s showed Streptococcus sensitive to co-amoxiclav
Imaging including xrays and scans
Summarise any imaging, such as CT, MRIs, or Xrays. Mentioning the date of imaging helps plan further imaging if needed. When mentioning the findings, highlight the impression from the report as well as any significant findings which was not mentioned in the impression section.
Many junior doctors often tend to read only the impression and can sometimes miss other significant findings, which may be unrelated to the request for the scan.
For example, you can see bowels loaded with faeces on a CXR and yet miss this finding. This is why you must make a habit of noting down the full report. Note that this can also include further follow-up imaging recommendations or next steps, as needed.
Step 9: Treatment Given and Course of Disease
Mention the treatment given, including antibiotics, fluids, oxygen, etc. and whether the patient improved or not (which is usually the case as in the discharge letter to GP).
A concise summary of key events is invaluable for GPs to understand hospital admissions and plan management accordingly.
- Medications given (especially antibiotics, fluids, steroids, insulin, etc.)
- Supportive care (e.g. oxygen, IV fluids, physiotherapy)
- Any procedures or surgeries performed
- Escalation or step-down decisions (e.g. switch from IV to oral antibiotics)
Example:
The patient was started on IV Co-amoxiclav and clarithromycin for pneumonia—required oxygen therapy initially, which was weaned off by Day 4. Antibiotics were switched to oral Co-amoxiclav to complete a 7-day course. Diabetes was managed with oral hypoglycaemics; no insulin needed.
You don’t necessarily need to mention specific details, such as what happened on which day. Instead, a concise idea of the course helps in getting a clear picture.
Step 10: Medication Changes and Further Follow-Ups
Medication Changes
You do not need to mention the antibiotic given on discharge, but this information can help if the patient is re-admitted shortly. Let’s say you started co-amoxiclav based on sensitivities, and you mention this in the NHS discharge letter.
The patient is re-admitted in 2 weeks. The clerking Doctor can read your discharge letter from the hospital and initiate co-amoxiclav treatment, as the patient responded well to it recently.
Other changes in the medications need to be mentioned as well, so the GP can understand who made the changes and why the changes were made.
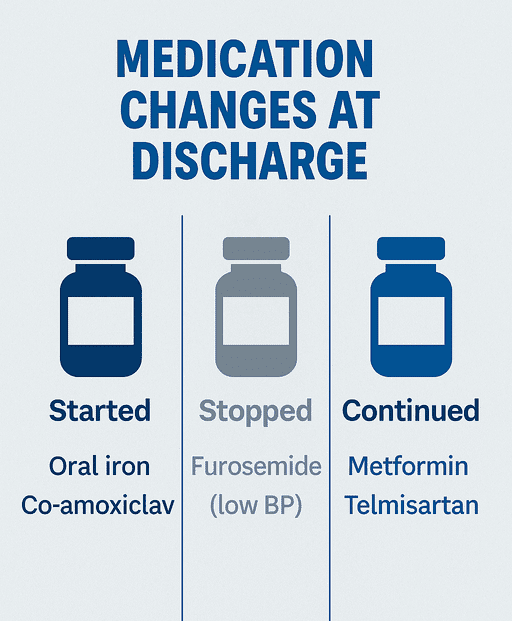
Example:
Furosemide was stopped due to low blood pressure
Oral co-amoxiclav for 5 days to complete a 7-day course of antibiotics
An oral iron supplement was started for a new case of iron deficiency anaemia
Further Follow-Ups
These can include follow-ups, outpatient investigations, or other speciality follow-ups. If appropriate, mention the specific date or a rough duration. If any scan is requested, please note the same as well.
Example:
OP Chest Xray in 4-6 weeks with OP Frailty Assessment Unit follow-up with the X-ray
Step 11: Diagnosis
I mentioned this section at the end because, in most NHS IT systems, it is typically located in a separate tab where you must enter the diagnosis.
Clearly state the primary diagnosis made during the admission using standard medical terms (e.g. “community-acquired pneumonia” rather than “chest infection”).
If the diagnosis is uncertain, you can write “suspected” or “working diagnosis” with a brief justification.
Example:
Community-acquired pneumonia Atypical chest pain
Note: Whenever possible, match the ICD-10 codes.
Step 12: Safety Netting, Notes to GP and Others
Use this section in discharge summary to provide clear instructions on what to watch for, who should act, and when to seek help.
- Safety netting means explaining what could go wrong and when to escalate — include red flag symptoms the patient should monitor (e.g. fever, SOB, confusion).
- Notes to the GP should include pending results, need for medication monitoring, repeat bloods, or follow-up reviews.
- Mention any social care, community teams, or referrals made (e.g. physio, SALT, district nurses), so the next clinician knows who’s involved.
Example:
GP to kindly monitor BP and restart anti-hypertensive medications as necessary.
District nurse referral for community TWOC in 1 week
Safety netting done, where the patient is advised to seek urgent help if shortness of breath worsens or new symptoms develop.
Conclusion
A clear, well-structured discharge letter is one of the most powerful tools you have to support safe, seamless patient care beyond the hospital.
By focusing on what truly matters — the diagnosis, treatment, follow-up, and red flags — you’re not only closing the loop but actively improving outcomes.
The goal is simple: help the next clinician pick up where you left off, without confusion.
And that, more than anything, is good medicine.

{kind=link}